MY PERSONAL EXPERIENCE OF PLAB 2
In my last post, I explained the basics of PLAB 2 in the simplest way possible. Now I am going into a bit deeper detail, throwing light on common myths and mistakes in PLAB 2 and tips to cope with them. It can be really helpful for the candidates who unfortunately failed their PLAB 2. But if you have not started preparing for PLAB 2, it’s natural that many of you guys won’t be able to apprehend it at the moment. My message to everyone is to go through this section again, once you have taken the PLAB 2 academy course. It will make more sense then.
COMMON MYTHS AMONG CANDIDATES
1. “All 3 sections of the station are judged independently.” There are 3 basic sections; data gathering, management and inter-personal (IP) skills. I’ll add another one here “time management”. Contrary to what other people say, I strongly believe that all four of them are highly interconnected and performance in one area will definitely affect your other sections. Just look at this picture: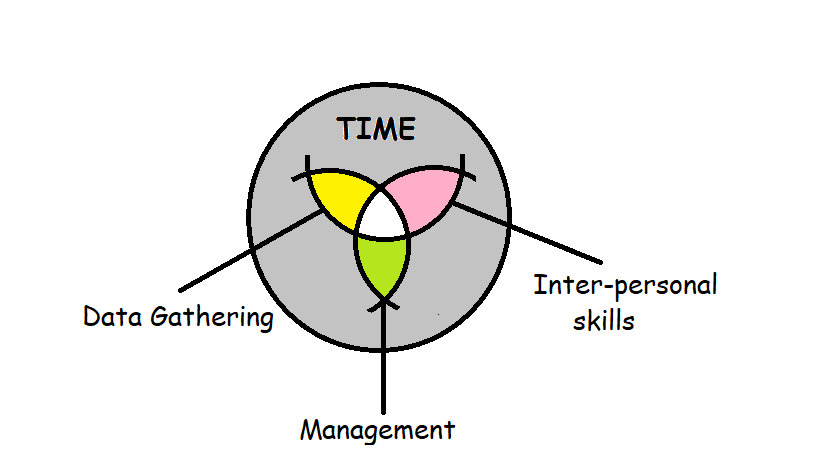
The white area in the middle represents your score. In order to succeed, you have to be an all-rounder. If your IP skills are weak, you will never get good marks in data gathering and management no matter how good you are in them. Similarly, if your IP skills are strong but you lack clinical knowledge, you will never get 4/4 in IP skills no matter what. Conversely, if you are good in all three of them but you don’t finish your station in time, there are chances you might still fail. BE AN ALL-ROUNDER!
2. “PLAB 2 is not a test of your knowledge, it’s a test of how you deal with patients” Partially contradict it. If you don’t have proper knowledge, how are you supposed to give proper consultation to the patient? For example, there is a pediatrics station in which a mother comes to you with her baby having tonsillitis. Now, if you don’t remember the ‘indications of tonsillectomy’ I assure you there is a high likelihood that you will never pass that station no matter how good your dealing with patients is.
3. “If a patient is happy with you at the end of the station, it means you have passed that station and vice versa” Absolutely incorrect. You will only pass if you have completed the task of the station regardless of the patient's attitude. For example, in my exam I got a station in which a lady had attempted a suicide by ingesting dozens of paracetamol pills; my task was to take relevant history, take blood sample (from a mannikin) and then manage the patient. I was sure I was going to fail that station because the lady did not cooperate at all (that was her role) but I passed anyway because I had completed the task. In the same way you can fail a station if you made your patient happy but didn’t complete the required task.
4. “If a patient does not want to talk, keep silent” There was a funny myth in our academy that once a student went into the station and the patient didn’t want to talk so, he kept silent the whole 8 minutes and when the result came, he had got 12/12 in that station 😛 All I can say is:

Look if a patient is not willing to talk, give him time, say words like “There is no rush, please take your time”, if he is crying, offer tissue, water etc. But you can’t afford to lose more than 1 minute in silence. Proceed with “I know you must be going through a lot, but I need to ask a few questions that might allow me to help you in a better way” and proceed with your task.
5. “You can still pass a station if your history taking was good but you made the wrong diagnosis.” You cannot pass that station, as simple as that. You will definitely get zero in management, 1 or 2 in data gathering (I am saying it because of my personal experience). In PLAB 2, you have to rule out all the differentials by your data gathering and give ONE SINGLE diagnosis to the patient and give him a management plan accordingly.
COMMON MISTAKES IN PLAB 2
1. “Time management” This is undisputedly, the most common cause of failure in the exam. Ask anyone who failed the exam, the most common answer will be, “I gave too much time to history taking and that left me very little time for clinical management.” A senior once said to me, “We Pakistanis have never been taught to take a proper history, so when we finally learn it, we get so excited that we unintentionally give all our time to history taking.” In my exam, there was a station of GCA (giant cell arteritis). Patient had vision loss. I had made my diagnosis in the 2nd minute when I asked her if it hurt when she combed her hair and chewed food and she said yes. But just to look cool in front of the examiner, I asked questions to rule out every single cause of vision loss on earth which took me too long. I had to do fundoscopy as well, which I did. In the end, I didn’t have enough time to talk about management plan. When results came, I had got 2 in history taking, 1 in management and 3 in IP skills. Even though I had taken such a long history, the examiner still gave me just 2/4. Why? Because I asked irrelevant questions and wasted time.
SUGGESTION: Try to finish history within 3-4 minutes. Be precise and concise. Try to start talking about clinical management as early as possible as it will allow your patient to ask more and more questions, hence more chances for you to score better in management and IP skills. If you haven’t started management and the 6-minute bell rings, just leave everything and move on to management.
2. “Too much and too little attention to IP skills and clinical knowledge, respectively” When we start our PLAB 2 preparation, the majority of us have good clinical knowledge but very little IP skills because we have never been taught that way. So naturally we start paying too much attention to IP skills and ultimately it destroys the balance between these two and ultimately leads to failure. Many times, our teachers tell us to not stick to notes too much and be natural. I personally am not in accord with this. I believe that we can stick to notes and still be natural as well. It’s all about practice.
SUGGESTION: Study your notes by heart. Keep your clinical knowledge updated. If you have enough knowledge, you will naturally feel at home with the given station and naturally in a position to answer patient queries in a better way. Having good IP skills is always a blessing. It does compensate for our lack of clinical knowledge a bit but it really can't compensate for lack of “basic” knowledge. Like I said earlier, if you don’t remember ‘indications of tonsillectomy’ in tonsillitis station, you will probably never pass it no matter how good your IP skills are.
3. “Fast Speech” A very common mistake among Asians, especially Pakistanis. I think we naturally have a fast way of speaking. Sometimes, if a station is long, we automatically start speaking fast so that we can complete the station. It’s a bad habit since we just keep talking and forget to listen to the patient. The examiners over there are very expert, they pick this up and cut our marks for being unprofessional.
SUGGESTION: Speak slowly, of course. While practicing with your colleagues, record yourself and listen to it later. If the station is long, try to be concise and precise instead of rushing through it. Listen to the patient carefully like you mean it. If a patient feels comfortable with you, he will literally help you with the station. For example, there was a TIA station. I finished the station in 7 minutes. The patient then asked, “Doctor, do you think I should drive?” And I said, “Oh, I am glad that you asked that question, I was just coming to that.” (I literally had forgotten that I had to forbid him from driving and tell him to go to DVLA, but he helped me with that himself.)
4. “Overconfidence” Another common reason for failure. Many times, you see people who did great in mocks, fail in the real exam and people who performed awfully in mocks, clear the exam. Doing good in mocks is a great feeling, it gives you good confidence to sit in the upcoming exam, however, there is a very thin line between confidence and over confidence, and if your cross it, it can lead to devastation. On the other hand, people who under perform in mocks can assess their weak areas in a better way and if they take the critical feedback constructively, they can easily turn the tables around in real exam.
SUGGESTION: Even if you are doing good in mocks, always go to your teachers and inquire them about your feedback. Ask your colleagues as well. Don’t get too chilled, little anxiety is always good for a good performance in the exam.
5. “Bad stations'' Everyone has some favorite stations and some “bad” stations. Sometimes we hate those stations so much that we don’t even bother to get better at them. We are like, “There are more than 350 stations, leaving just a few ones won’t be such a bad idea.” But hey, I swear it is. 😛 There is an obstructive uropathy station, in which you have to take history about BPH, pass Foley catheter and tell management plan to patient. I hated that station to my guts, because unlike in Pakistan, urinary catheterization is a very technical procedure in the UK. It came in my mock and I failed it. Still, I didn’t bother to learn from my mistakes. Ironically, it came in my real exam as well and as soon as I entered the room and saw the apparatus, I knew I was gonna fail that one and I did, miserably.
SUGGESTION: Like they say, “Keep your friends close and your enemies closer.” Enough said 😀
No comments:
Post a Comment